

Schizophrenic Constellations
Schizophrenic Constellations
The super-programmes the brain puts in place to keep us alive

SPECIAL PHYSIOLOGY
The subject I am about to introduce in this article is something totally new to me. I delved into the infinite world of Germanic Medicine a few years ago and still observe my surroundings on a daily basis with what I have often called 'the spectacles of the five biological laws'. I can no longer watch a film or TV series without encountering those biological processes that I am so passionate about. Someone will think I have a few screws loose and who knows, maybe that someone might even be right. However, as my friend Federico Franco said in an interview a few months ago, these laws teach us how to live, so I can't help but savour their essence in every second of my life.
It is not an obsession, but rather a simple awareness of something that exists regardless of whether I notice it or not. If nature has provided me with tools that are always accessible, free and verifiable, why should I preclude myself from using them?
When we delve into the universe of the five biological laws, we realise that the relationship between the psyche - i.e. he or she who inhabits that marvellous biological container that is the body - the brain - i.e. the CPU that governs how we respond to everyday events - and the organ - the target of the biological programme - are inseparably linked. We have learnt how each event perceived by the individual as acute, isolated, dramatic and shocking activates a programme on these three levels, shaping what is called a 'biological programme in special physiology'.
Every time we have to text on the phone, lock the door, water a plant or stroke the cat, we are in 'normal physiology'. The difference between the two is very simple. In normal physiology, there is a desire, i.e. the practical and material manifestation of a need - no matter what the magnitude - and consequently an action through which the subject achieves that particular 'goal'. Shall I lock the door? I turn the key in the lock. Do I have to shoot a penalty? I take my run-up and shoot. I have to go shopping? I start the car and drive to the supermarket. Normal physiology therefore moves according to the following procedure:
Desire
Action
Satisfaction/fulfilment

Please note. Whenever we have to perform an action such as those described above, we are always going to activate one or more parts of the brain. In the example of the key in the lock, we are going to activate the brain areas that regulate the function of the muscles of the arm and hand that we will use to turn the key. In the case of the penalty shot, I will activate all the areas that allow me to make the movements necessary to shoot that penalty shot and score the goal. At the moment I write this article, I am activating certain areas of the brain in normal physiology, otherwise I would not be able to tap my fingers on the computer keyboard. In all these cases, the brain produces current, estimated at around 250 nA. This is a very slight electrostatic field that must be grounded by the performance of an action.
To understand in a very simple way what happens in our brain, you have to imagine lightning striking a house. That lightning bolt is desire. Every house - at least in today's societies - is equipped with an earthing system for the current. If this system were not in place, the electricity from the lightning would discharge onto the appliances, creating electrostatic fields like those created in our brains. Earthing, in this case, is what corresponds to the above-mentioned 'action'.
What happens instead when the action is missing? A real electrochemical imbalance takes shape within our brain, starting with the acute, isolated, dramatic and shocking event (DHS). Being in special physiology, the electrostatic field that is formed in the vicinity of a certain area can reach up to 3000/3500 nA and all this happens when we are faced with a 'non-action'. It is as if instead of shooting the penalty shot, I freeze in front of the penalty spot.
As has already been explained in numerous previous articles, these processes also lead to a modification - or imbalance - at an organic level, both from a functional and an anatomical point of view. The mass of the affected tissue will be altered - it increases in the active phases of the palaeo-brain programmes and decreases in the active phases of the neo-brain programmes - and will increase in function in accordance with the biological conflict that the individual experiences from the DHS. Until now, the programmes I have mentioned in my articles on the five biological laws all referred to these types of activations. In reality, special physiology can also manifest itself through a more complex form of biological activation. These are what Hamer called 'schizophrenic constellations', that series of physiological manifestations that conventional medicine categorises as 'psychic illnesses'.
Megalomania, mythomania, bulimia, anorexia, and asthma are some of the examples of these 'super-special' programmes, but before we get into the heart of the matter, it is worth emphasising once again that these are survival mechanisms that our brains put into action in situations of extreme emergency. If the concept was not clear, constellations serve to keep the individual alive!
Does this sound strange? Let's find out why, starting as always with the basics.
I AM CONSTELLATED!
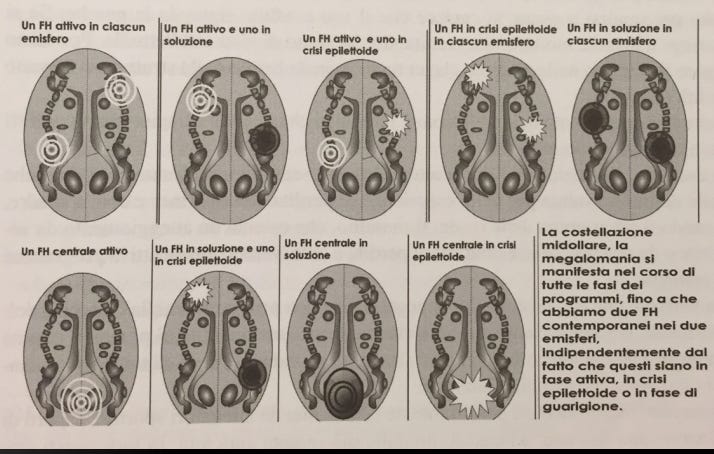
A schizophrenic constellation takes hold when there are two or more activations involving both cerebral hemispheres, or two areas far enough apart to constitute a magnetic polarity. The situations currently verified are as follows:
Two active foci (activated brain areas)
One active focus and one in epileptoid crisis
Two foci in epileptoid crisis
One central conflict engaging both hemispheres (also in epileptoid crisis)
Only in the white matter - which regulates tissues derived from the recent mesoderm - can there be two foci in solution (PCLA) or a single central foci in solution
Attention: activations always concern the same embryonic leaflet, but it is not excluded that several constellations relating to different embryonic leaflets may coexist. Example: if I have activated the lung (endodermis-trunk) and at the same time I have also activated the interstitial tissue of the left testicle (recent mesoderm-midgut) I am not in a schizophrenic constellation. Otherwise, I could activate lung and intestine (endodermis-tronchus) and at the same time activate left testicle and right testicle (recent mesoderm-midgut). In the latter case I am faced with a double constellation of endoderm and recent mesoderm respectively.
I reproduce below some notes taken from the slides of the Human Biology course, as I believe they can be of enormous help in understanding the subject:
The number of constellations is infinite. Hamer says he has observed more than 500 of them
Each one of us has, at every moment of life, a highly personal brain activity, given by the set of active conflicts, EC and PCLA: this set constitutes the emotional, psychic and physical appearance/arrangement of the person
Every 'illness' must be understood and embedded within the constellation(s) the person is experiencing at that moment
This makes it all the more futile to try to fit all patients with a similar 'illness' within a statistic, each case is unique
CONSTELLATION OF THE ENDODERM: THE DISMAYED
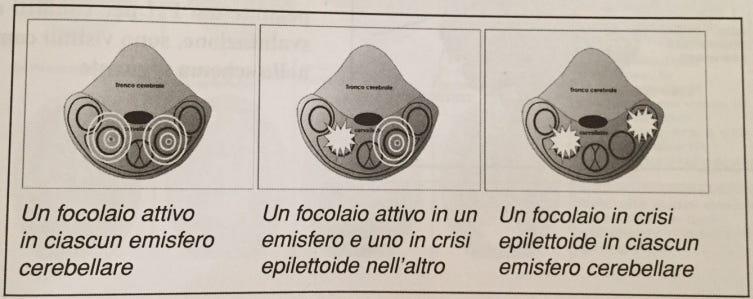
With regard to the constellations of the brainstem and thus of the endodermis, these always activate with an active focus in one hemisphere and one in epileptoid seizure in the other, or two in active phase, or two in epileptoid seizure (see picture at the end of the paragraph).

This constellation is also referred to as the 'conflict of the ebetes', as the typical symptoms are feeling disoriented, lost, dismayed and confused. One can also think of the figure of the zombie, i.e. an individual who walks very slowly, at a snail's pace, without realising why he or she is in a certain place or situation and sometimes without even the perception of being alive.
The survival super-programme that the brain puts in place has the sense of keeping the individual still while waiting for the situation to evolve, as at that moment he is unable to swallow or expel any vital morsels. Another symptom that can evoke this constellation is the divergence of the eyes, almost as if the dismayed individual is under the effect of a spell. We must remember that the endoderm speaks to us of vital needs, so the brain's objective is to raise protection levels as high as possible in order to ensure the organism's vital processes run smoothly.
Once out of the state of consternation, the subject is slightly inebriated, as if he has just emerged from a kind of hypnosis. He has totally lost contact with reality. It is a very frequent constellation in all those individuals who feel they have lost all perspective related to life, such as the elderly in a hospice, prisoners or those diagnosed with a terminal illness.

CONSTELLATION OF THE ARCHAIC MESODERM: THE EMOTIONAL DEAD
In the cerebellum the dynamics of the foci is exactly the same as in the brainstem and the respective activations are not 'altered' at the level of the organic mass. The characteristic feature of this constellation is emotional death, which can manifest itself in asocial behaviour, absence of stimuli or desires. One tends to be apathetic with little energy.

It is also possible to manifest atypical behaviour, such as disrespectful or rude jokes. It is easy to confuse an emotional dead person with a depressive, even though the aetiology is totally different. On the contrary, it is also possible for the emotionally dead person to put himself or herself at the disposal of everyone, with the desire to play the part of the 'good Samaritan'. An example of this constellation is embodied in the figure of Mother Teresa of Calcutta.
CONSTELLATION OF THE RECENT MESODERM: MEGALOMANIA
Megalomania is perhaps the schizophrenic constellation that everyone, even the uninitiated, has heard of at least once in their life. The marrow super-programme has the sense of leading the individual to regain self-esteem. The area involved tends to correspond to the part of the body that one wants to enhance the most.

This is the programme of the "Rambo" or "Super-man". A megalomaniac feels exalted, is present, focused, feels unassailable and full of strength. He is also arrogant, boastful and always wants to prevail over others. Again, the brain's goal is not to suspend the symptoms and activations that gave rise to the super-programme, in fact no symptoms are perceived. The brain's only goal is to put the subject in a position to climb back up the slope and give himself a new value.
THE CONSTELLATIONS OF THE ECTODERM (CORTEX)
The cerebral cortex is the part of the brain that differs the most from other mammals, particularly in terms of size. In terms of schizophrenic constellations, we are entering a veritable universe of variables and conditions that has yet to be fully discovered in the state of the art.
Hamer has identified some 500 constellations of the cortex and of course it becomes impossible to list them all, besides the fact that it would be quite presumptuous on my part, as the subject is still being studied and explored. As I already mentioned in a previous article, the cortex can be subdivided into several 'sections', each with their respective super-programmes. Below is a quick list of all the constellations of the cortex, but I will not go into them further, at least not in this article. The subject is so vast that each individual super-programme would deserve at least a whole article, so I will limit myself to briefly listing the categories of interest to us:
Motor cortex constellations
Constellations of the sensory cortex
Constellations of the post-sensory cortex
Constellations of the basal cortex
Constellations of the frontal cortex
Constellations of the occipital cortex
Constellations of the peri-insular or hormonal cortex
Constellations in the cortical areas of blood-glucose regulation
Constellation of the thalamus
In the next articles I will begin to develop my thoughts on some of these constellations, primarily those concerning the hormonal cortex, since some of them are already covered in previous articles. Stay tuned.
NEURO-DEGENERATIVE DISEASES (BUT IS IT REALLY SO?)
Although not necessarily related to the constellations of the cortex, it is necessary to open a parenthesis on those activations that for so-called 'traditional' medicine are considered 'neuro-degenerative diseases' and that affect brain areas of the cortex. Alzheimer's, Parkinson's, diabetes all the way to asthmatic states, panic attacks and glaucoma. This is another piece to be added to the immense subject of constellations, as they can often be found as a consequence of an ongoing cortical constellation or, on the contrary, can also represent its incipit.
One thing that is certainly worth dwelling on at this juncture is the fact that these are not actually incurable diseases from which it is impossible to escape or alleviate their symptoms. You have to consider that in the collective imagination these types of programmes are seen as a slow and inexorable descent into hell. A road with no escape routes or secondary exits. For example, the moment an Alzheimer's diagnosis is presented, measures are put in place that inevitably lead the subject to lose confidence in regaining their memory skills.
As if this were not enough, to make the diagnosis even worse, the social context also comes into play, as those close to him will begin to treat him as if he actually had 'something wrong', marking his defective situation. This starts by using phrases such as 'don't you remember me telling you this before?', or 'have you forgotten already?' and the like.
This series of attitudes, added to possible conflicts of the kidney collectors (refugees) that biologically increase the symptoms of any kind of activation, can only keep the subject in a constant state of alarm, precluding any possibility of improvement.
The same thing applies when removing a teaspoon from the hand of a subject with Parkinson's symptoms. "Don't worry dad, I'll do it for you" or "you risk dropping everything on the floor, let me clear the table". Just imagine the amount of conflict an individual can experience when the thought is instilled in him that he is unable to do something and that the condition will only get worse. A real vicious recurring cycle.

It is of course not my purpose to criticise those who do this, also because it is certainly always for the good, but the reason why I, along with many other better and more experienced disseminators than myself, engage in the dissemination of this knowledge is also to make the users aware of the existence of such programmes, without the presumption of wanting to save the world. I will be sure to go into more detail on this subject as well, but for now I feel I must stop here. The topics are many and I would risk confusing ideas by putting too much meat on the fire. In the meantime, I look forward to the next article.